Research Article - Der Pharma Chemica ( 2018) Volume 10, Issue 7
Seroprevalence Study of Whooping Cough in National Institute of Hygiene, Rabat, Morocco During 2013-2017
Meryem Elgarini1,2*, Abderrahmane Hammoumi1, Zakaria Mennane2, Aicha Qasmaoui2 and Reda Charof2
1Department of Biology, Faculty of Sciences Ain Chock, Laboratory of Microbiology, Pharmacology, Biotechnology and Environment, University of Hassan II Km 8 Route d’El Jadida, B. P 5366 Maarif Casablanca 20100, Morocco
2Department of Bacteriology, Laboratory of Epidemic Diseases, National Institute of Hygiene Avenue Ibn Batouta, Rabat, Morocco
- *Corresponding Author:
- Meryem Elgarini
Department of Biology
Faculty of Sciences Ain Chock
Laboratory of Microbiology, Pharmacology, Biotechnology and Environment
University of Hassan II Km 8 Route d’El Jadida
B. P 5366 Maarif Casablanca 20100, Morocco
Abstract
Background & objectives: Pertussis is a bacterial respiratory infection caused by the Bordetella pertussis and Bordetella parapertussis. B. pertussis-specific antibodies can be detected by enzyme-linked immunosorbent assays (ELISAs). The antigens most frequently used as pertussis toxin (PT). The objective of this study is to determine whooping cough by enzyme immunoassay ELISA IgM.
Methods: Antibodies IgM response to pertussis toxin was measured by enzyme-linked immunosorbent assay in 16 cases. Cases suspected with clinical symptoms typical of whooping cough and family contacts of children with pertussis were referred to The Laboratory of epidemic diseases in the National Institute of Hygiene, Morocco.
Results: Out of 16 suspected cases, 4 (25%) were positive, 8 (50%) were negatives and 4 (25%) were doubtful.
Interpretation & conclusions: The serology is particularly valuable for the diagnosis of pertussis is sensitive and specific and its sensitivity is not amended by the antibiotic, contrary to the culture and PCR, and is useful for the diagnosis in the case of investigations around a case of whooping cough or the date of the declaration of the disease is late to carry out the PCR technique. Our study carried out between 2013 and 2017 allowed us to note that the main contaminant is the members of the family.
Keywords
Bordetella pertussis, Elisa, Pertussis toxin, Serology, Whooping cough.
Introduction
Pertussis or whooping cough is a bacterial respiratory infection caused by the gram-negative bacteria Bordetella pertussis and B. parapertussis, B. bronchiseptica and B. can also cause the disease in humans [1-3]. Pertussis is an important cause of morbidity and mortality in infants worldwide. Vaccination programs led to decline many pertussis cases and deaths among children. Pertussis vaccine (combined with diphtheria and tetanus toxoids) has been used in Morocco in the National immunization program since its beginning in 1980 [4,5].
The disease is notifiable in many countries. Worldwide, there are an estimated of 16 million cases of pertussis, 95 % of which occur in developing countries, resulting in about 195 000 children deaths per year [3,6] According to World Health Organization, the disease associated with nearly 63 000 deaths among children aged <5 years in 2013, although there is considerable uncertainty over these estimates in view of the paucity of reliable surveillance data, particularly from developing countries [4].
Before vaccination program, each two to five years, an outbreak related to whooping cough affecting many children, mainly children under 5 years. Vaccination will reduce these incidences, however vaccine do not prevent the disease due to circulation of B. pertussis [7,8]. Several factors contribute to the persistent of this circulation, therefore, the immunity decline after 4-12 years from immunization [9] other factor related to genetic changes in the pathogen led to many cases in immunized peoples in different countries [10].
Diagnosis of pertussis based on clinical symptoms is complicated due to the misdiagnosis and wide spectrum of symptoms similarity to many infectious diseases [11]. Culture, molecular techniques like polymerase chain reaction (PCR), and serology techniques, are the most diagnostic tools for identification and surveillance. The choice of diagnostic method differs depending on the phase of the disease and age [6,12].
B. pertussis-specific antibodies can be detected by enzyme-linked immunosorbent assays (ELISAs) or multiplex immunoassays, which use one or mixed antigens. The antigens most frequently used are pertussis toxin (PT), filamentous haemagglutinin (FHA), pertactin (PRN) and fimbriae (FIM). Sometimes, adenylate cyclase-haemolysin toxin (ACT) is also used. In routine diagnosis, only the measurement of anti-PT antibodies is recommended because they are specific for B. pertussis, and the cross-reacting antigens have not been described. Whereas anti-FHA, anti-PRN, anti- FIM and anti-ACT are less specific due to cross-reactivity with other microbial antigens (other Bordetella species, Haemophilus species, Mycoplasma pneumoniae, Escherichia coli) [13-15].
The objective of this study is to determine whooping cough by enzyme immunoassay ELISA IgM among sera of suspected cases and family contacts referred to The Laboratory of epidemic diseases, National Institute of Hygiene Rabat, Morocco, during 2013-2017.
Materials and Methods
Sera
During March 2013 and December 2017, 16 sera from suspected cases of pertussis and sera of the investigation around a case of Pertussis conducted by the Directorate of Epidemiology and fight against the disease referred to The Laboratory of epidemic diseases, National, Institute of Hygiene Rabat, Morocco. The age of the patients: 1 new-born (age : 16 days), 7 infant (median age, 2 months, range 1-5 months), 5 children (median age, 10 years, range 5-15 years) and 3 adults (median age, 45 years, range 37-60 years).
Enzyme-linked-immunosorbent assay
IgM antibodies to pertussis toxin in serum simples is measured by an enzyme-linked-immunosorbent assay (Novalisa™ B. pertussis/IgM ELISA) the assay was performed according to the manufacturer’s instructions described previously. For IgM tests the serum specimens were diluted 1+100 with IgM sample diluents. 100 μl from diluted serum, cutoff, positive and negative control was added to pertussis toxin antigen-coated micro wells and incubated for 1 hour at 37 ± °C. When incubation has been completed, remove the foil and wash each well three times with 300 μl of Washing Solution. Dispense 100 μl of pertussis toxin anti-IgM Conjugate into all wells except for the Blank well and incubate for 30 min at room temperature. When incubation has been completed, remove the foil and wash each well three times with 300 μl of Washing Solution. Dispense 100 μl of TMB (Tetramethylbenzidine) Substrate Solution into all wells and incubate for 15 min at room temperature in the dark. Dispense 100 μl of Stop Solution into all wells and measure the absorbance of the specimen at 450/620 nm within 30 min after addition of Stop Solution.
Results and Discussion
B. pertussis is a human pathogen which causes whooping cough, an endemic illness responsible of morbidity and mortality, particularly in infants under 6 months old. In literature, paroxysmal cough is considered the most important classical symptom of pertussis, it is also a major criterion in clinical case definitions of World Health Organization and Center for Disease Control and Prevention [16]. In this study all patients had clinical signs of pertussis evolving since last a week; these straights were followed by inspiratory recovery in singing of Coq in 18% of cases. Of access of cyanosis and apnea, have been observed (Table 1).
| Clinical signs | Percentage |
|---|---|
| Productive cough | 23% |
| cough | 39% |
| Apnea | 15% |
| Cyanosis | 15% |
| Inspiratory recovery in | 15% |
| Singing of Coq |
Table 1: Percentage of clinical signs
IgM antibodies
Our study documented 16 cases with clinical symptoms in favor of Pertussis between 2013 and 2017: We have identified 4 children of 16 have positive serology (25%), 8 cases have a negative serology (50%), with 4 doubtful cases (25%) (Figure 1). The sex ratio is 0.23 and the ages ranging from 16 days to 60 years it is different to the results of the study carried out by the laboratory of epidemic diseases, National, Institute of Hygiene Rabat, Morocco between 2008-2012 they found a percentage of 58 % positive case of Pertussis [17].
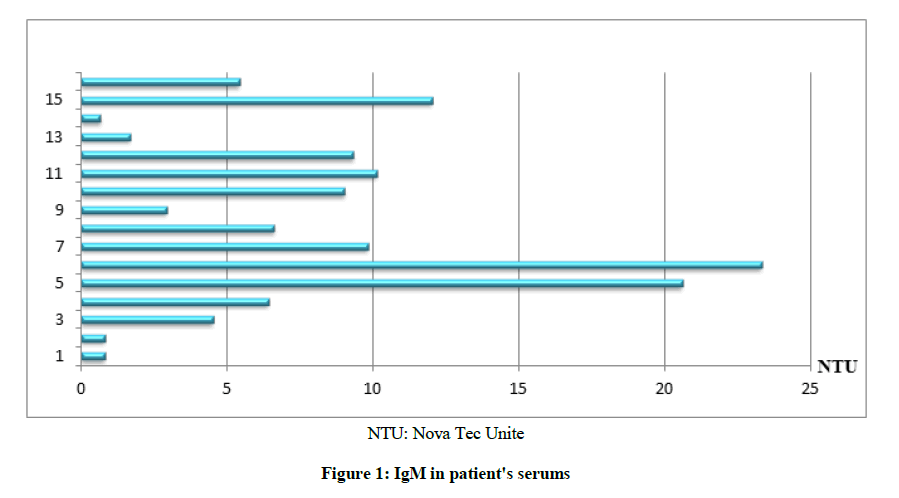
Figure 1: IgM in patient's serums
For doubtful cases this does not rule out the possibility of a pertussis at its onset, a second sample must be taken after 15 days from the date of the first sample. Paired sera were not studied in this work. For the negative cases this does not draw aside the possibility of a whooping-cough at is beginning with negative IgM, or the cases with infection due to Bordetella parapertussis had no antitoxin response but causing clinical symptoms compatible with a diagnosis of pertussis [18,19]. Antibodies of IgM class are known to exist only transiently in the early phase of the immune response. Thus, the demonstration of specific IgM permits the laboratory diagnosis of infectious disease from one serum specimen for cases have positive serology [20].
Vaccine status in patients
Despite good vaccination coverage, it is estimated that 50 million cases occur each year, with approximately 300000 deaths annually, 90% of them in developing countries [21]. Moroccan children are vaccinated against pertussis with a cellular vaccine at the age of 2, 3, 4 months, first rappel of 18 months and second rappel of 5 years a major contribution to reducing infant and child mortality, which decreased by 86% for pertussis in children aged 1 to 12 months [22]. In our study, 2 out of 16 cases were not immunized, 4 were not have age of vaccination, 6 were not completely vaccinated, 2 is vaccinated and no information on vaccination status was available for 2 patients (Figure 2).
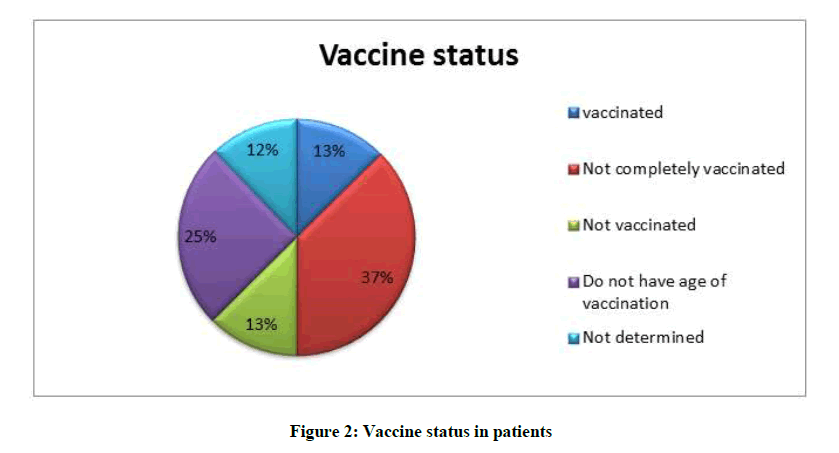
Figure 2: Vaccine status in patients
In Morocco the whooping-cough is a notifiable disease, in 1987, 1078 of case of Whooping-cough are declared with a vaccine cover of 85% to the DTC. The incidence rate passed from 76.9 per 100000 inhabitants in 1980 to 0.30 per 100000 inhabitants in 1990 thanks to the widened program of vaccination set upin 1980, the continuous incidence rate to decrease to arrive at 0.08 per 100000 inhabitant sin 2000 and 0.05 per 100000 inhabitants in 2010, but a resurgence at observed, 331 cases in 2012 with an incidence rate which reaches 1.0 per 100000 inhabitants [23-26]. The sera referred to The Laboratory of epidemic diseases, National, Institute of Hygiene between 2008-2012 is 48 cases and 16 cases between 2013-2017, does not mean a decrease in pertussis cases but because of a change in the method of diagnosis which is based on the PCR-RT and culture on the middle of Bordet gengou. The causes of this disease resurgence are still unclear. Some hypotheses raised were include a circulation of B. pertussis among adolescents and adults, from these groups, the infection of infants who are not fully immunized; implementation of molecular methods for diagnosis; improvement of epidemiological surveillance systems; or even genetic changes in the pathogen [22,16].
Conclusion
In conclusion, the serological test is more useful for the diagnosis of the disease in the case of investigations around a case of whooping cough or the date of the declaration of the disease is late to carry out the PCR technique. Our study carried out between 2013 and 2017 on the suspect cases and the family contacts allowed us to note that the main contaminant is the members of the family.
References
- Y.V. Lobzin, I.V. Babachenko, O.V. Shamsheva, A.A. Tetenkova, N.V. Bakhareva, V.P. Boitsov, N.N. Zvereva, Infect. Dis. Ther., 2015, 4, 113-123.
- L.M. Guimaraes, BMC Infect. Dis., 2015, 15(442), 1-12.
- R. Muloiwa, B.M. Kagina, M.E. Engel, G.D. Hussey, System. Rev., 2015, 4(62), 1-7.
- Weekly epidemiological record, WHO, Geneva, 2015, 35(90), 433-460.
- M.T. Lahrech, News of vaccinations in Morocco, 25-27 December 1987, Tangier Morocco: Moroccan Society of Medical Sciences, 1988, 306.
- I. Pavic-Espinoza, S. Bendezú-Medina, A. Herrera-Alzamora, P. Weilg, M.J. Pons, M.A. Aguilar-Luis, V.P. Helasvuo, M. Juana del Valle a, BMC Infect. Dis., 2015, 15, 554, 1-7.
- I. Crespo, N. Soldevila, P. Munoz, P. Godoy, G. Carmona, A. Dominguez, BMC Public Health., 2014, 14, 268, 1-7.
- N. Benamrouche, M. Lazri, S. Mahrane, R. Ouraghi, D. Touati, K. Rahal, Biological Diagnosis of Pertussis Algeria. Ministry of Health, Population and Hospital Reform, Directorate General for Prevention and Promotion of Health, 2013.
- W. Hellenbrand, D. Beier, E. Jensen, M. Littmann, C. Meyer, H. Oppermann, C.H. Wirsing von König, S. Reiter, BMC Infect. Dis., 2009, 9, 22, 1-11.
- D.N. Fisman, P. Tang, T. Hauck, S. Richardson, S.J. Drews, D.E. Low, F. Jamieson, BMC Public Health., 2011, 11, 694, 1-10.
- M.L. Von Linstow, P. Lotko Pontoppidan, C.H. Wirsing von König, J.D. Cherry, B. Hogh, Eur. J. Pediatr., 2010, 169, 1119-1122.
- L. Knorr, J.D. Fox, P.A.G. Tilley, J. Ahmed-Bentley, BMC Infect. Dis., 2006, 6(62), 1-12.
- N. Guiso, G. Berbers, N.K. Fry, Q. He, M. Riffelmann, C.H. Wirsing von König, Eur. J. Clin. Microbiol. Infect. Dis., 2011, 30, 307-312.
- Q. Zhang, H. Zheng, M. Liu, K. Han, J. Shu, W. Chenggang, X. Ning, H. Qiushui, L. Huiming, BMC Infect. Dis., 2012, 12(138), 1-7.
- M. Elgarini, A. Hammoumi, Z. Mennane, A. Qasmaoui, R. Charof, Int. J. Innov. App. Studies., 2016, 416-424.
- G.V.D. Brink, J.O. Wishaupt, J.C. Douma, N.G. Hartwig, F.G.A. Versteegh, BMC Infect. Dis., 2014, 14(526), 1-10.
- M. Elgarini, A. Hammoumi, Z. Mennane, A. Qasmaoui, H. Oukouchoud, C.H. Ounaim, R. Charof, Int. J. Innov. App. Studies., 2016, 18, 2, 408-415.
- M. Granström, G. Granström, P. Gillenius, P. Askelöf, The J. Infect. Dis., 1985, 151, 4, 646-649.
- G. Zackrisson, I. Krantz, T. Lagergatrd, P. Larsson, R. Sekura, N. Sigurs, J. Taranger, B. Trollfors, Eur. J. Clin. MicrobioL Infect. Dis., 1988, 149-154.
- M.K. Viljanen, O. Ruuskanen, C. Granbergl, T.T. Salmp, Scand. J. Infect. Dis., 1982, 14, 117-122.
- R.S. Torres, T.Z. Santos, R.A. Torres, V.V. Pereira, L.A. Fávero, O.R. Filho, M.L. Penkal, L.S. Araujo, J. Pediatr. (Rio J), 2015, 91, 333-338.
- K. Lahlou, National Immunization Program: Evolution and Prospects. Population Directorate, Ministry of Health, Kingdom of Morocco, 2017.
- P.D. Compaore, Epidemiological, clinical and therapeutic study of whooping cough in the pediatric department at the University Hospital of Marrakech from 2009 to 2011. Thesis Medicine, Marrakech: Cadi Ayyad University Faculty of Medicine and Pharmacy Marrakech, 2012, 85.
- Directorate of Planning and Financial Resources Division of Planning and Studies Department of Studies and Sanitary Information, Health in numbers 2012, Kingdom of Morocco: Ministry of Health, 2013, 179.
- State of health of Moroccan population. Kingdom of Morocco: Ministry of Health, 2012.
- M.T. Lahrech, News about vaccinations in Morocco, 25-27 Décembre, Tanger, 1987.



